
Spouses and children can be greatly affected by these invisible injuries and their side effects. How? A spouse may become a “caregiver” and have to abandon the role as wife or husband, in order to deal with the daily crisis resulting from untreated PTSD, while a child, whose parent has PTSD, may develop anxieties and self-esteem issues.
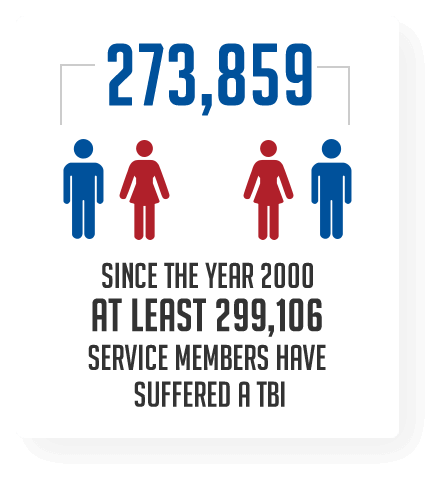
Mild Traumatic Brain Injury in SM is typically the result of direct blunt trauma to the head or blast injuries. The resulting effects of these are displayed over the course of time. Anywhere from immediately after the injury or, they may begin to demonstrate the signs days or weeks after the injury. Some signs of mTBI are, being dazed, confused, or disoriented. A person does not have to lose consciousness to incur mTBI. Other signs include issues with memory, concentration, balance, blurred vision, sensitivity to light, speech, and mood changes. Historically, the effect of these brain injuries will be all encompassing of one’s life. As with PTSD, the individual, family, and work life all suffer as a result of the changes to the person’s capability, which is why education is a key factor. ORWF provides the tools for individuals to learn how to cope with mTBI, understand it, and make changes to adapt and get stronger.
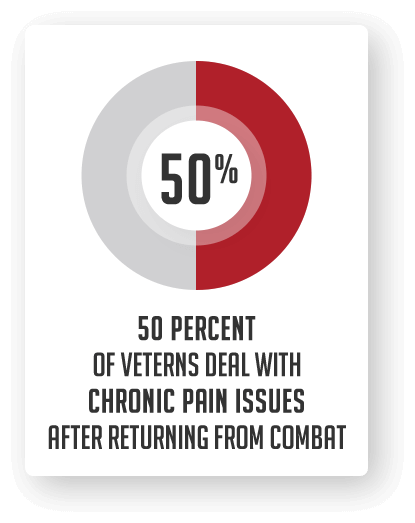
Spouses and family members, working on coping with their loved one’s chronic pain can be exhausting. The added pressure of “invisible pain” that is often not diagnosed by physicians can be extremely difficult and leave people feeling hopeless. There are new options and ongoing research treatments available for a variety of pain issues.
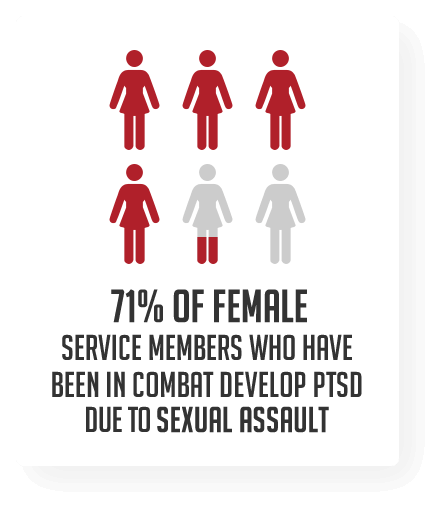
Post-Traumatic Stress Disorder (PTSD) is the common result of any sexual assault and within the military community the level of trauma is compounded. MST survivors face a long and painful recovery and need the support of the military community as well as the civilian community to overcome their psychological injuries.
The stress on military families from overseas deployments is immense. When a service member is deployed, the separation can be lonely and difficult for both the service member and his or her spouse. As challenging as being apart can be, however, coming home often involves hard realities as well. This is especially the case when a spouse is severely injured. The pressure of coping with wartime injuries is often a cause of military divorce. The sheer number of soldiers who have returned from Iraq or Afghanistan suffering from Post-Traumatic Stress Disorder (PTSD) and other related problems is undeniable.
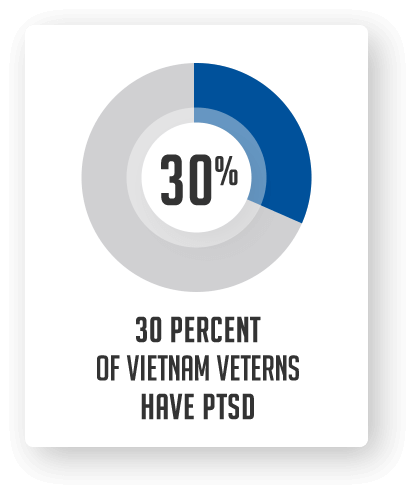
PTSD also takes a toll on marriages and other relationships. For example, research has found that 38 percent of “Vietnam veteran marriages failed within six months of the veteran’s return from Southeast Asia.” Research also finds that “veterans with PTSD are more likely to report marital or relationship problems, higher levels of parenting problems, and generally poorer family adjustment than veterans without PTSD.” A 2005 Pentagon study found that the divorce rate for Iraq and Afghanistan veterans was up 78 percent since 2003.

